Chronic care management is care coordination services done outside of the regular office visit for patients with. A personal health assistant is assigned to the senior to help develop and manage a care plan keep track of medications and facilitate appointment setting follow up to ensure the senior receives coordinated care in between doctor visits.
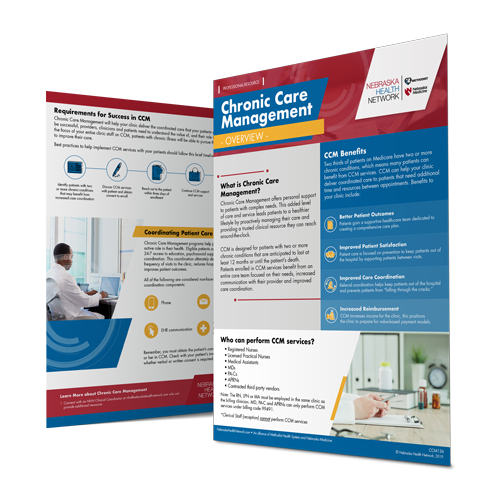
 Chronic Care Management Patients Nebraska Health Network
Chronic Care Management Patients Nebraska Health Network
Chronic Care Management CCM is a Medicare service for beneficiaries with two or more chronic conditions such as diabetes and hypertension.

Chronic care management patient brochure. Chronic care management benefits a practice by increasing the quality of care for patients dealing with two or more chronic conditions. Chronic Disease Management Patient Information PDF 385 KB If you have difficulty accessing the PDF please contact the MBD webmaster Summary. Chronic care management services to you.
The only fear that providers are running into is that they worried about the time and effort it will take to. In addition to office visits and other face-to face encounters which must be billed separately these services include communication with. 20-60 minutes of care coordination per month.
In addition to office visits and other face-to-face encounters billed separately these services include communication with the patient and other treating. Chronic care management allows the patient to be more involved and connected to the healthcare team. Chronic Care Management CCM Our Turnkey CCM Offering.
The Chronic Care Model defines the care delivery system components that support care delivery for patients with chronic illnesses. What are the Outcomes. Completed remotely in addition to regular office visits.
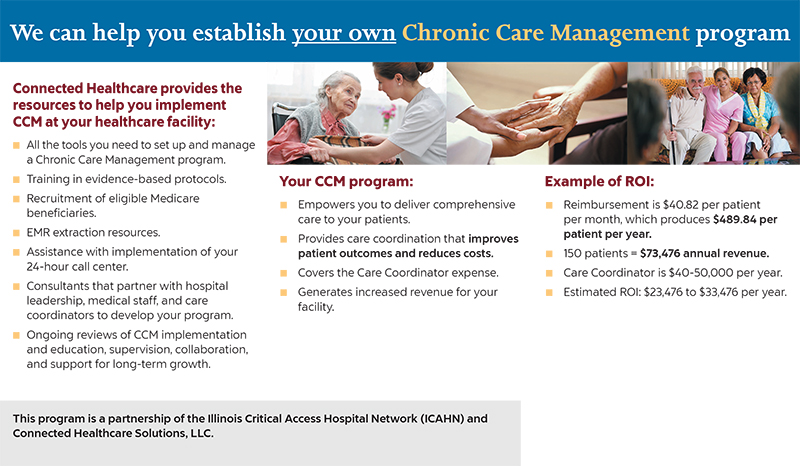
The Centers for Medicare Medicaid Services CMS now reimburses practices approximately 43 per patient per month for providing non-face-to-face chronic care management CCM for Medicare patients with two or more. Guided by the development of a care plan. CareVitality optimizes your existing technology to document CCM services in your existing EHR and provides 247365 nursing services.
Download patient tools such as food and exercise diaries a chronic pain medication agreement and a new patient welcome letter. Doctors now HOW to treat chronic disease but dont know WHEN. The lack of care coordination and disease management The lack of patient-centered care.
Chronic Care Management Overview Chronic Care Management CCM is defined as the non-face-to-face services provided to Medicare beneficiaries who have two or more significant chronic conditions. Chronic care management services may include. Chronic Care Management CCM is defined as the non-face-to-face services provided to Medicare beneficiaries who have multiple two or more significant chronic conditions.
The Connected Care initiative provides resources and tools that can help health care professionals learn how to implement chronic care management CCM and receive payment for providing these services. 3 Control Cost Drivers 3 Improve Health Outcomes and Patient Satisfaction 3 Drive Long-Term Behavior Change. What are the Benefits.
Several of these components or services have been incorporated into Medicares CCM service such as self-management support and clinical information systems to enhance self-care care coordination and. What are the Challenges. Chronic care management CCM is defined as.
The CMS 2017 CCM Rule was created to help physicians address the needs of Medicare patients with multiple chronic conditions. Personalized assistance from a dedicated health care professional who will work with you to create a care plan. 247 emergency access to a health care professional.
Manage chronic conditions and help organizations reduce overall costs. One in four adults still live with multiple chronic conditions and most of it requires daily management. Coordination of care between your pharmacy specialists testing centers hospitals and more.
Principal Care Management PCM Our Turnkey PCM Offering. Chronic care management CCM is non face-to-face care coordination services done outside of the regular office visit for patients with multiple two or more chronic conditions expected to last at least 12 months or until the death of. Chronic care management is designed to help optimize patient care outside the clinic or hospital premises.
CareVitality provides the most comprehensive care management solutions and additional Healthcare IT consulting to help put you on a successful road map to participating in value-based care under MACRAQuality Payment Program QPPMIPSAPM. Medicare considers patients eligible for chronic care management if they have multiple two or more chronic conditions. Chronic Care Management Personalized interventions to help individuals better.
Patients spend on average only 5 hours a year in the doctors office. Many Medicare recipients are eligible to receive these additional benefits. We need better patient-centered coordinated care covering that time patients are NOT in a doctors office.
At least 20 minutes a month of CCM services. Return to main toolbox page Chronic Care Management Patient Letter. Medicare defines a chronic condition as a condition that is expected to last for at least 12 months and that increases the risk of death acute.
What is CCM CPT Code 99490. It also brings a new stream of revenue as well as a new patient base into any medical practice. Chronic Care Management 101.
CCM services are only available to patients with two or more chronic conditions. There are two types of plans that can be prepared by a General Practitioner GP for Chronic Disease Management CDM. Medicare developed the Chronic Care Management program to assist patients and their families in receiving comprehensive support to treat their chronic medical conditions.
The Chronic Care Management Resource.
![]() Ccm
Ccm
 Flyer Brochure Medicare Chronic Care Management Display Advertising Png 870x450px Flyer Advertising Advertising Agency Brand Brochure
Flyer Brochure Medicare Chronic Care Management Display Advertising Png 870x450px Flyer Advertising Advertising Agency Brand Brochure
 What Is Chronic Care Management
What Is Chronic Care Management
Https Www Nachc Org Wp Content Uploads 2019 03 Care Management Action Guide Mar 2019 Pdf
 Final Carter Healthcare Brochure 2
Final Carter Healthcare Brochure 2
 Chronic Care Management Nebraska Health Network
Chronic Care Management Nebraska Health Network

 Chronic Care Management Offers Challenges Opportunities For Physicians
Chronic Care Management Offers Challenges Opportunities For Physicians
.5x11-01.png) Chronic Care Management The Evolution In Continuity Of Care Sidney Regional Medical Center
Chronic Care Management The Evolution In Continuity Of Care Sidney Regional Medical Center
 Chronic Care Management Ccm Catalina Island Medical Center
Chronic Care Management Ccm Catalina Island Medical Center
 Winter 2017 January March By Missouri Academy Of Family Physicians Issuu
Winter 2017 January March By Missouri Academy Of Family Physicians Issuu
 Csc Chronic Care Management Teahutt Creative
Csc Chronic Care Management Teahutt Creative





No comments:
Post a Comment
Note: Only a member of this blog may post a comment.